New York Medicaid Exclusion Screening Requirements
What are the exclusion screening requirements for New York Medicaid providers?
New York Medicaid providers must screen all employees, vendors, and contractors against the New York State Exclusion List and the Office of the Medicaid Inspector General Exclusion List of Excluded Individuals and Entities prior to hire and monthly as a condition of participation. Providers must also document their screening with detailed exclusion check reports. (Source: Original Webpage)
How often must New York Medicaid providers conduct exclusion screening?
Providers are required to review the New York State Office of the Medicaid Inspector General Exclusion List and the Human Services Office of Inspector General’s List of Excluded Individuals and Entities at least every thirty (30) days. (Source: Original Webpage)
What are the consequences of failing to screen for exclusions in New York Medicaid?
Failure to screen can result in overpayment liability, penalties, and exclusion or termination for providers. Reimbursements made in violation of the payment prohibition are considered overpayments and must be repaid. Liability for overpayments attaches to the provider, the party that caused the claim, and anyone who received payment. Civil money penalties can reach up to ,000 per item, or ,000 for repeat violations within five years. (Source: Original Webpage)
Which exclusion lists must New York Medicaid providers check?
Providers must check the New York State Exclusion List, the Office of the Medicaid Inspector General Exclusion List, the federal OIG’s List of Excluded Individuals and Entities (LEIE), and, in many cases, the GSA/SAM and other state exclusion lists. (Source: Original Webpage)
How do New York Medicaid exclusion lists differ from federal exclusion lists?
New York’s exclusion list is separate from and independent of the OIG’s LEIE. Many individuals on New York’s exclusion list are not on the LEIE, and vice versa. For example, only 58% of nurses and 40% of doctors on New York’s list were also on the LEIE, based on sample comparisons. (Source: Original Webpage)
What types of conduct can lead to exclusion from New York Medicaid?
Conduct such as employing excluded parties, submitting claims on behalf of excluded parties, accepting payment for services provided by excluded parties, submitting false claims, making false statements, soliciting bribes or kickbacks, and providing unnecessary medical care can lead to exclusion. (Source: Original Webpage)
Are exclusions automatically imposed for unacceptable practices in New York Medicaid?
No, exclusions are not automatically imposed. The Department of Health may choose to impose lesser penalties, such as limitations on participation or censure, depending on the facts and circumstances. (Source: Original Webpage)
What documentation is required for exclusion screening in New York?
Providers must document their screening activities with detailed exclusion check reports, which serve as evidence of compliance with screening obligations. (Source: Original Webpage)
What are best practices for exclusion screening in New York?
Best practices include screening all employees, vendors, and contractors prior to hire and monthly; documenting screening with detailed reports; adding disclosed entities to routine monthly exclusion lists; and screening the GSA/SAM and other state lists in addition to the NY List and LEIE. (Source: Original Webpage)
How do Medicaid Managed Care Organizations (MMCOs) affect exclusion screening obligations?
MMCOs contractually impose screening obligations on participating providers, requiring them to screen employees, subcontractors, temporary workers, volunteers, and sub-delegates against federal and state exclusion lists every month. (Source: Original Webpage)
Do private payers require exclusion screening for New York Medicaid providers?
Yes, most private payers require providers not to employ or contract with any employee, subcontractor, or agent who has been debarred or suspended by the federal or state government, or excluded from participation in Medicare or Medicaid. Initial applicants must not be federally sanctioned, debarred, or excluded from participation in Medicare, Medicaid, or FEHBP. (Source: Original Webpage)
What is the impact of New York’s payment prohibition on excluded parties?
The payment prohibition means that New York Medicaid will not reimburse any items, services, or supplies furnished, ordered, or prescribed by an excluded provider. Any activity related to medical care or services provided by an excluded party is banned, and reimbursements made in violation are considered overpayments. (Source: Original Webpage)
How does exclusion screening affect provider enrollment in New York Medicaid?
Providers must disclose owners, agents, and managing employees during enrollment and certify under penalty of perjury whether any have been excluded, revoked, or terminated from any healthcare programs under Medicare, Medicaid, or Social Services. The requirement extends to laboratory directors, supervising pharmacists, and anyone with operational or managerial control. (Source: Original Webpage)
Are providers required to screen disclosed entities monthly?
Yes, it is a best practice to add disclosed entities to the routine monthly exclusion list, ensuring ongoing compliance with screening obligations. (Source: Original Webpage)
What happens if a person is on the LEIE but not on the New York Medicaid Exclusion List?
Being on the LEIE does not guarantee inclusion on the New York Medicaid Exclusion List. Samples showed only 58% of nurses and 40% of doctors on New York’s list were also on the LEIE. Providers should screen both lists to ensure compliance. (Source: Original Webpage)
If I’m on the New York Exclusion List, will I also be added to the OIG Exclusion List?
It depends. When a State excludes or sanctions a provider, it must notify the OIG, which evaluates whether a federal exclusion is warranted. For example, exclusion for failing to pay State taxes may not result in federal exclusion, but exclusion for healthcare fraud would. (Source: Original Webpage)
If I’m on the New York Exclusion List, will I be added to other State lists?
Maybe. States are required to notify their sister states when they exclude a provider for cause, so other states can evaluate whether to impose exclusion under their rules. Compliance with this regulation is improving over time. (Source: Original Webpage)
Features & Capabilities
What services does Exclusion Screening offer to support compliance?
Exclusion Screening offers employee screening, vendor and contractor screening, a compliance hotline, proprietary SAFER™ software for automated exclusion screening, and white label services for partners and resellers. (Source: Knowledge Base)
How does Exclusion Screening’s SAFER™ software improve compliance?
The SAFER™ software automates exclusion screening, provides daily updates, uses advanced algorithms to handle inconsistent data formats and duplicate names, reduces false positives and negatives, and scales to organizations of any size. (Source: Knowledge Base)
Does Exclusion Screening offer vendor and contractor screening?
Yes, Exclusion Screening verifies that vendors and contractors are compliant, helping organizations reduce regulatory risks and maintain compliant business relationships. (Source: Knowledge Base)
What is the Compliance Hotline and how does it help?
The Compliance Hotline is a secure and anonymous channel for employees and partners to report fraud, waste, and abuse, fostering a culture of integrity and early issue detection. (Source: Knowledge Base)
How does Exclusion Screening minimize false positives and negatives?
Exclusion Screening uses advanced algorithms and resolution-focused screening, confirming identities with multiple data points to reduce false positives and negatives. (Source: Knowledge Base)
Pain Points & Solutions
What compliance challenges do healthcare organizations face?
Healthcare organizations face complex compliance processes, manual screening challenges, regulatory risks, fraud detection needs, cost-effectiveness concerns, legal risks, and resource management issues. Exclusion Screening addresses these with automation, advanced algorithms, vendor screening, and secure reporting channels. (Source: Knowledge Base)
How does Exclusion Screening help organizations avoid penalties?
Exclusion Screening’s resolution-focused screening ensures thorough and accurate checks, helping organizations avoid penalties such as Civil Monetary Penalties (CMP) by confirming identities and maintaining compliance. (Source: Knowledge Base)
How does Exclusion Screening save organizations time and resources?
By automating the screening process with SAFER™ software, Exclusion Screening saves organizations significant time and resources, allowing them to focus on their core operations. (Source: Knowledge Base)
How does Exclusion Screening address fraud detection and reporting?
Exclusion Screening provides a Compliance Hotline for secure and anonymous reporting of fraud, waste, and abuse, enabling early detection and resolution of compliance issues. (Source: Knowledge Base)
Use Cases & Benefits
Who can benefit from Exclusion Screening’s services?
Healthcare providers, compliance officers, risk managers, legal teams, operational managers, hospitals, clinics, healthcare networks, and organizations with extensive vendor relationships benefit from Exclusion Screening’s tailored solutions. (Source: Knowledge Base)
Is Exclusion Screening suitable for small practices?
Yes, Exclusion Screening offers cost-effective and scalable solutions tailored to the needs of small practices, automating compliance processes and saving time and resources. (Source: Knowledge Base)
How does Exclusion Screening support large healthcare systems?
Exclusion Screening’s SAFER™ software scales to handle high volumes of screenings efficiently, provides vendor and contractor screening, and manages frequent database changes with advanced algorithms and daily updates. (Source: Knowledge Base)
What business impact can organizations expect from using Exclusion Screening?
Organizations can expect improved compliance, cost savings, operational efficiency, risk mitigation, enhanced integrity, scalability, and legal and financial protection. (Source: Knowledge Base)
Pricing & Plans
How is Exclusion Screening’s pricing determined?
Pricing is competitive and customized based on the specific monitoring lists and the volume of screenings required. This tailored approach ensures cost-effectiveness and scalability for organizations of all sizes. (Source: Knowledge Base)
How can I get a quote for Exclusion Screening’s services?
You can receive a personalized quote by filling out the form on the contact page. The team will reach out to demonstrate the solution and discuss pricing details. (Source: Knowledge Base)
Competition & Comparison
How does Exclusion Screening differ from other exclusion screening providers?
Exclusion Screening stands out with its proprietary SAFER™ software, resolution-focused screening, expertise of former Federal prosecutors, comprehensive services, cost-effectiveness, scalability, and commitment to clients. (Source: Knowledge Base)
Why choose Exclusion Screening over competitors?
Exclusion Screening offers daily updates, advanced algorithms, resolution-focused screening, legal expertise, comprehensive services, competitive pricing, scalability, and time/resource efficiency, making it a preferred choice for reliable and legally sound exclusion screening solutions. (Source: Knowledge Base)
Technical Requirements & Implementation
How long does it take to implement Exclusion Screening’s solution?
New clients can get started and begin screening within 1 day, which is faster than many other vendors. (Source: Knowledge Base)
How easy is it to start using Exclusion Screening?
Exclusion Screening’s SAFER™ software is designed for seamless integration, automating the exclusion screening process and eliminating the need for extensive manual effort or technical expertise. Dedicated support from compliance specialists ensures a smooth setup. (Source: Knowledge Base)
Product Information & Authority
Who founded Exclusion Screening and what is their expertise?
Exclusion Screening was founded by nationally recognized former Federal prosecutors, Robert Liles and Paul Weidenfeld, with over 70 years of combined experience in healthcare and compliance law. (Source: Knowledge Base)
What is Exclusion Screening’s vision and mission?
Exclusion Screening aims to be a national leader in exclusionary screening, providing competitively priced services accessible to organizations of all sizes. Its mission is to simplify compliance processes, mitigate legal risks, and support healthcare providers in focusing on their core operations. (Source: Knowledge Base)
Are there any case studies demonstrating Exclusion Screening’s impact?
Yes, Exclusion Screening provides a case study on the impact of a False Claims Act judgment on OIG exclusions, highlighting compliance challenges and the importance of thorough exclusion screening. Read the full case study here. (Source: Knowledge Base)
Which industries are represented in Exclusion Screening’s case studies?
The laboratory services industry is represented in Exclusion Screening’s case studies, specifically a Texas-based laboratory services company involved in submitting false claims. (Source: Knowledge Base)
Does Exclusion Screening provide guides for Medicaid screening obligations in other states?
Yes, Exclusion Screening offers guides for Apple Health providers in Washington, assisting with exclusion and sanction screening obligations for any role affecting Medicaid billings or deliverables. Access the guide here. (Source: Knowledge Base)
New ReportScreening Failures & Their Financial Fallout — $26M in penalties and how to avoid them. Download the report →
A Provider’s Guide to New York Medicaid Exclusion Screening
This article focuses on helping providers understand New York Medicaid exclusion screening law, and its exclusion screening requirements so that they can avoid the risks associated with employing or doing business with excluded parties.
A Provider Guide to New York Medicaid Exclusion Screening
The New York Medicaid Program is prohibited by State law from paying for items or services furnished excluded parties. The State ban, which is separate and independent of federal law, is enforced primarily through mandated provider exclusion screening requirements and the threat of imposing overpayment liability, penalties, and exclusion or termination for providers that fail to screen and violate the payment ban. This article focuses on helping providers understand New York Medicaid exclusion screening law, and its exclusion screening requirements so that they can avoid the risks associated with employing or doing business with excluded parties.
New York Determines Who Can Provide Services to its Medicaid Program
New York is responsible for the administration of its Medicaid program. It sets the standards and qualifications for its participating providers and is authorized to exclude providers from participation if the action is supported by either State or Federal law. The State ensures that its participating providers have not been excluded from participation in State or Federal health care programs through the enactment and enforcement of exclusion screening rules and obligations.
Basis for Exclusion in New York
Exclusions are imposed in New York for engaging in “unacceptable practices under the medical assistance program.” This includes employing excluded parties, submitting claims on behalf of excluded parties, and accepting payment services provided by an excluded party as the basis for an exclusion. Other conduct that is considered an unacceptable practice includes, but is not limited to, submitting false claims, making false statements in support of a claim, soliciting bribes or kickbacks, and providing unnecessary medical care. Federal Exclusions imposed by the Office of Inspector General are a separate basis for exclusion under State law.
Conduct that constitutes an unacceptable practice under the medical assistance program violates the conditions of participation in the Medicaid program, however sanctions are based on the underlying conduct and exclusions are not automatically imposed. The Department of Health can choose to impose lesser penalties, such as limitations on a provider’s participation or censure, if the conduct does not, it its view, warrant exclusion.
The New York Medicaid Exclusion List
The New. York Medicaid Exclusion List is a registry of the individuals and entities that the State Department of Health has excluded from participating in the State Medicaid. The list is maintained by New York’s Office of the Medicaid Inspector General and hosted on its website,
The difference in exclusion lists is highlighted by the fact that there are many people on New York’s Exclusion list who are not on the LEIE; the reverse is also true. For example, when a random (though not statistically valid) sample of LPNs, RNs and CNAs on the New York were compared to the LEIE, it was found that only 58% were also on the LEIE. And when a a random (though again not statically valid) sample of physicians on the New York list were compared with the LEIE, just 40% of the doctors on New York’s List were also on the LEIE. The most likely explanation for this discrepancy is that New York excluded these individuals for reasons that would not support a federal exclusion, but regardless of the reason, it is important that providers be aware of these large differences. Particularly when doing exclusion screening!
The Impact of the State’s “Payment Prohibition”
The New York Medical Assistance Program will not reimburse any items of medical care, services or supplies furnished, ordered or prescribed an excluded provider. The ban extends to any activity, whether direct or indirect, relating to medical care or services being provided and to all forms of payment. As previously stated, submitting claims for services provided by an excluded party is, in of itself, a basis for exclusion. In addition, any reimbursements made in violation of the payment prohibition are overpayments which must be repaid, and liability for overpayments attaches to the provider that submits the claim, to the party that caused the claim to be submitted, and to anyone that received payment. In addition, all of those mentioned above are jointly and severely liable for repayments of the overpayments.
Excluded parties that order, provide or prescribe care services or supplies are also subject to civil money penalties up to $10,000 for each item that is paid if there have been no violations within the last five years. If there has been a prior violation within the previous five years, the department may impose a penalty of up to $30,000. The department considers the damage to the program, the facts and circumstances and any mitigating factors in setting the penalties.
Talk to a compliance specialist today
For the past 12 years our exclusive mission has been to remove the burdens of complexity and support compliance with CMP laws. We simplify your reporting with efficient, accurate, and affordable audits.
Providers need to be aware that their exclusion screening obligations arise from different sources and for different reasons. For example, the State requires screening as a condition of payment and as part of the enrollment process – but the requirements for each as different. Screening obligations are also imposed contractually by Medicaid Managed Care Organizations (MMCO) and by Private Payers, and these can also vary. After a review of the requirements New York providers face, we will suggest some provider “best practices.”
Enrolled providers are required to implement and maintain effective compliance programs with policies and procedures that confirm the identity and exclusion status of their employees. In determining the exclusion status of a person, providers “shall review” the New York State Office of the Medicaid Inspector General Exclusion List and the Human Services Office of Inspector General’s List of Excluded Individuals and Entities “at least every thirty (30) days.” Providers must also be prepared to document their screening with detailed exclusion check reports.
Exclusion Screening Obligations as Part of Enrollment
Providers must enroll in New York’s medical assistance program in order to be eligible to receive payments for items or services they provide. To enroll, providers must disclose its owners, agents and managing employees, and certify under penalty of perjury whether any have been excluded, revoked, or terminated, from any health care programs under title XVIII (Medicare), title XIX (Medicaid) or title XX (Social Services) of the Social Security Act.
The enrollment screening requirement poses two issues. First, the disclosure categories are defined broadly to include laboratory directors and supervising pharmacists and “anyone who exercises operational or managerial control over or who directly or indirectly conducts the day to-day operation” in addition to the owners, agents and managers. Second, the requirement, as written, extends beyond the State List and the LEIE to other State and federal exclusion lists!
Exclusion Screening for Participating Providers in Medicaid Managed Care
Medicaid Managed Care Organizations are required to determine the exclusion status of their participating providers and its subcontractors and to require them to comply with the exclusion status requirement. They meet this by contractually imposing screening obligations on their participating providers. Although each MMCO has its own contract, the following excerpt is typical of the obligations that are imposed:
[Payer] also requires you not employ or contract with any employee, subcontractor or agency who has been debarred or suspended by the federal or state government, or otherwise excluded from participation in the Medicare or Medicaid programs…
First-tier, downstream and related entities (FDRs), must review federal (HHS-OIG and GSA) and state exclusion lists before hiring/contracting employees (including temporary workers and volunteers), the CEO, senior administrators or managers, and sub-delegates. Employees and/or contractors may not be excluded from participating in federal health care programs. FDRs must review the federal and state exclusion lists every month…
As can be seen, this MMCO contract broadly defines who must be screened (it includes temporary workers, volunteers and subcontractors). It adds the federal General Services Administration/System for Awards Management List (GSA/SAM) in addition to the LEIE, and, as written it requires that the screening of all state lists in addition to the New York list.
Exclusion Screening Required by Private Payers
Most private payers also will not pay for services furnished by excluded parties. The following language, taken from one of the private payers, is commonly found in provider manuals:
We require that providers not employ or contract with any employee, subcontractor or agent who has been debarred or suspended by the federal or state government, or otherwise excluded from participation in the Medicare or Medicaid program…Initial applicants …must not be currently federally sanctioned, debarred, or excluded from participation in any of the following programs: Medicare, Medicaid or FEHBP…
These requirements by this private payer are similar to the MMCO contractual requirements in that it also seems to extend the obligation beyond those of the State by clearly including the GSA/SAM and seemingly including all State lists.
Suggested Provider Best Practices
Providers are required to screen all employees, vendors and contractors with the New York State Exclusion List and the Office of the Medicaid Inspector General Exclusion List of Excluded Individuals and Entities prior to hire and monthly as a condition of participation,” so this is clearly should be the starting point for all screening programs.
Providers should also document their screening with detailed exclusion check reports.
Since providers are required to screen the parties identified in their disclosure obligation and certify their exclusion status, it is a best practice to add the disclosed entities to the routine monthly exclusion list.
In light of the MMCO and enrollment requirements, Providers are best served if they also screen the GSA/SAM and the other State Lists in addition to the NY List and the LEIE,,
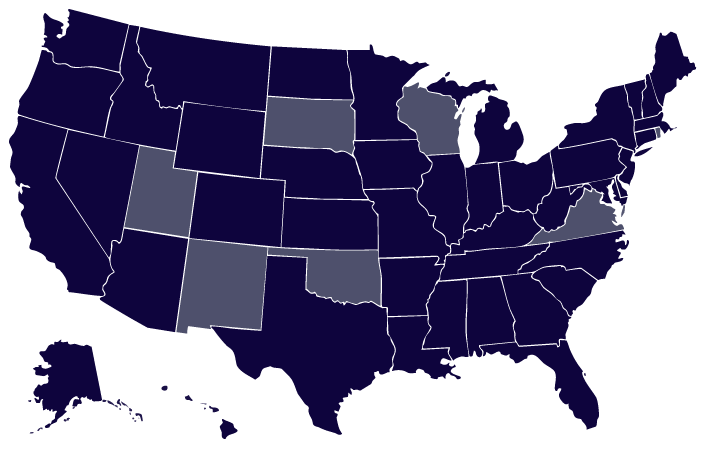
Map of the States with a Separate Medicaid Exclusion List and Article
Current States With a Separate Medicaid Exclusion List
The focus of this article is to help providers identify which States have a separate Medicaid exclusion list, how they are different from the federal exclusion lists, and the effects on screening.
Some Frequently Asked Questions
If a Person is in the LEIE, Will he always be in the New York Medicaid Exclusion List?
Not necessarily. Even though an OIG Exclusion is a “mandatory exclusion” under State law18 NYCRR § 515.8(1), a large number of New Yorkers are on the NY Exclusion List but not on the LEIE. As mentioned earlier, samples of nurses showed that only 58% of nurses on the NY List were also on the LEIE, and only 40% of the doctors on New York’s List were on the LEIE! Regardless of the cause of these differences, they provide strong support for screening both exclusion lists.
If I’m on the New York Exclusion List, will I also be added the OIG Exclusion List?
It depends. When a State excludes or sanctions a provider, it is required to notify the OIG so that it can evaluate the facts and circumstances and decide whether a federal exclusion is also warranted. For example, an exclusion for failing to pay State taxes might be appropriate under state law, but the OIG could not impose a federal exclusion on that basis. On the other hand, a State exclusion based on a healthcare fraud conviction in State Court would clearly support a federal exclusion, and the OIG would seek a federal exclusion upon notification of the action.
If I’m on the New York Exclusion List, will I be on Added to Other State Lists?
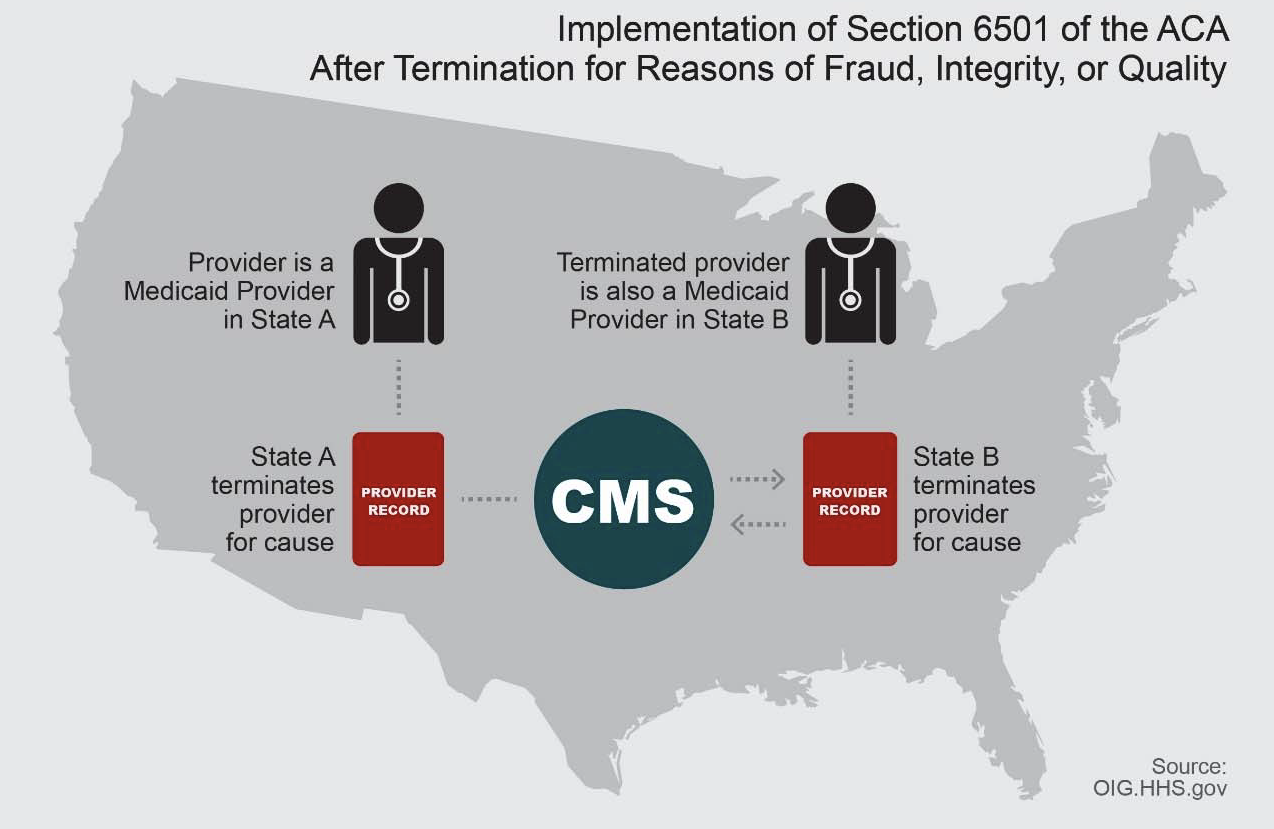
Again, the answer is Maybe. States are also required to notify their sister States whenever they exclude a provider “for cause” so that they, like the OIG, can evaluate whether or not to impose an exclusion pursuant to their rules. An exclusion “for cause” is one that is based on actions that the State believes would also be the basis of a federal exclusion. The diagram below shows how the process is supposed to work.
As described by CMS in guidance to the States, the implementation of section 6501 of the ACA involves three steps: First, a State agency must communicate to its sister states about providers who have been excluded, or terminated, for cause; second, the agency must identify whether any of those providers are participating in the State’s Medicaid program; and, third, the agency must exclude or terminate the provider’s participation in its own State Medicaid program if appropriate under its rules of participation. Compliance with this regulation and guidance is sporadic among the states, but it continues to improve and get better over time.
FinalThoughts
Providers in New York have exclusion screening obligations from multiple sources, and the only way to meet them is by having a robust exclusion screening program. The best program for each provider regarding “who to screen” and “what databases to screen” will depend on a number of factors, such as the payer requirements and their relationship to claims, but providers are urged to carefully consider these questions in terms of risks and benefits.
Related Resources
State Databases
Map of all states with separate Medicaid exclusion lists we screen against.