
We are sometimes asked, “Why do you screen against the National Plan and Provider Enumeration System...

The OIG’s November 2023 Compliance Guidance The OIG’s November 2023 Compliance Guidance lists 7 elements...

This article focuses on helping providers understand New York Medicaid exclusion screening law, and its...
Alabama’s Medicaid Program will not pay for any item or service furnished by, or at the medical direction...
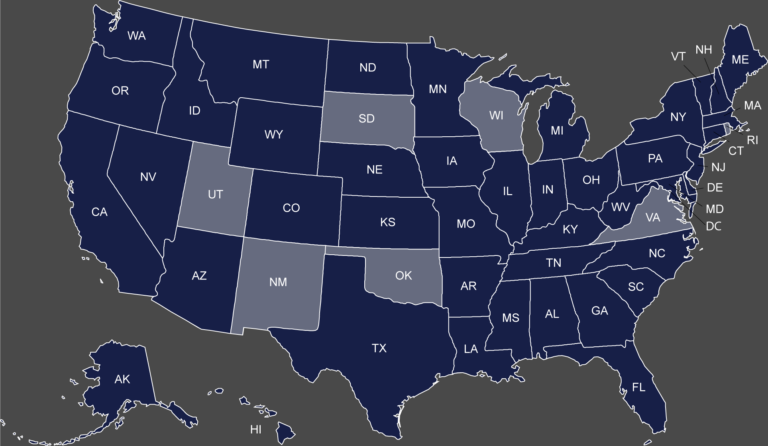
Map of the States with a Separate Medicaid Exclusion List Click on your state to view their Medicaid...
OIG Exclusion List vs. CMS Preclusion List Since the CMS Preclusion list was announced in April 2018,...
We have previously discussed that once a provider is excluded he may not furnish items or services...
What are the California Exclusion List Screening requirements? The Medi-Cal Program will not pay...

The Pennsylvania Precluded Provider List, commonly referred to as “Pennsylvania Medicheck ,” identifies...

Exclusions and debarments are powerful administrative sanctions imposed by Federal and State agencies....
The importance of screening employees, vendors and contractors against available federal and State exclusion...

Most healthcare providers and suppliers in the State of California are aware that exclusions imposed...

A Provider’s Guide to OIG Exclusions: Federal Exclusion Regulations and Enforcement Authorities, and...
OIG Exclusions are powerful enforcement sanctions that bar an individual or entity from any participation...

At Exclusion Screening, we often receive questions about the scope and frequency of an organization’s...

I. Introduction The Office of Inspector General (OIG) has the authority to exclude providers from participating...

The last two years have been rough for everyone, and it has been particularly difficult for healthcare...

The Centers for Medicare and Medicaid Services (CMS)[1] is the Federal agency tasked with the overall...

Medicare and Medicaid providers / suppliers are prohibited from employing individuals who have been excluded...
To understand the North Carolina Exclusion Screening Requirements, we must first touch upon Exclusions...
I. What is the NPDB The National Practitioner Data Bank (NPDB) was created as part of the Health Care...
The Department of Health and Human Services (HHS), Office of Inspector General (OIG) is responsible for...
The Department of Health and Human Services (HHS), Office of Inspector General (OIG) exercises both mandatory...
Exclusion Actions Under 42 U.S.C. § 1320a-7(b)(5)(B) (November 2020): Since 1976, the Department...

The Department of Health and Human Services (HHS), Office of Inspector General (OIG) may be required...
After finding a confirmed exclusion among your employees, vendors, contractors, or volunteers there are...
Massachusetts Medicaid Exclusion Screening: Requirements and Best Practices for Compliance The Massachusetts...
Should you choose to participate in the Medicare and/or Medicaid programs, you must comply with a wide...
Over the past year, both State and Federal law enforcement investigators and prosecutors have gone to...
The Office of Inspector General (OIG) recently published its Semi-Annual Report to Congress covering...
(May 2, 2019) The Alabama Medicaid Program imposes significant exclusion screening requirements on its...
(April 4, 2019): In December of 2018 a study was conducted by Kyle Wench (George Washington University)...
(April 2, 2019) The Department of Health and Human Services (HHS), Office of Inspector General (OIG),...
(March 1, 2019) The Department of Health and Human Services (HHS), Office of Inspector General (OIG),...
Beginning April 1, 2019, the new CMS Preclusion List will go into effect subsequently barring many healthcare...
By Cason Liles (February 6, 2019): The Department of Health and Human Services (HHS), Office of...
(February 6, 2019) The Department of Health and Human Services (HHS), Office of Inspector General (OIG),...
(December 17, 2018): Texas Medicaid Exclusions will prevent the Texas Medicaid Program from...
(August 23, 2018): In 2008, after learning that a Texas-based laboratory services company was submitting...
Perhaps the most severe administrative sanction available under the Social Security Act stems from the...
(January 22, 2018): With 2017 behind us, it can be quite helpful to review the Medicare “exclusion”...
(January 12, 2018): The Medicare and Medicaid programs are both essential, yet costly health benefit...
(January 8, 2018): Most physicians will progress through their entire career without ever having...
Year in Review OIG Podcast Earlier this week, the Office of Inspector General released its “Year in Review”...
(August 16, 2017): Earlier this summer, the U.S. Department of Justice (DOJ) executed its most extensive...
The Office of the Inspector General (OIG) has recently entered into a number of exclusion case settlements tied...
Exclusion News (May 22, 2017): By Paul Weidenfeld Health Care Fraud will continue to be a high priority...
The recently issued Resource Guide for Measuring Compliance Program Effectiveness, reconfigures the traditional...
By Paul Weidenfeld The new Final Rule issued by CMS revising the conditions of participation for home...
In what appears to be a growing enforcement trend, the Department of Health and Human Services, Office...
Exclusion Violation by Dentist “Sends a Strong Warning” February 1, 2017 By Paul Weidenfeld...
By Paul Weidenfeld January 23, 2017 On January 12, 2017, the Office of Inspector General published a...
DOJ Announces $4.7 billion in FCA Recoveries By Paul Weidenfeld December 16, 2016 The “Third Best...
OIG Imposes Record $21.5 Million in Penalties for Exclusion Violations! The OIG imposed a record $21.5...
[1] The Office of Inspector General (OIG) has steadily increased its enforcement of OIG Exclusion Screening...
By Robert W. Liles. August 3, 2016. The False Claims Act is the primary...
On April 18, 2016, the Department of Health and Human Services, Office of Inspector General (HHS-OIG)...
I. The OIG Reinstatement Process Most exclusions are imposed for a definite time period. The question...
By Paul Weidenfeld, March 4, 2016. An essential element of all compliance plans is developing and...
The Office of Inspector General’s 2016 OIG Work Plan contains two important projects that focus...
In August, we discussed an OIG audit, which revealed that Medicaid providers who were terminated for...
The failure to report excludable offenses by state Medicaid offices and licensing boards is a longstanding...
In February, we reported that the Michigan Attorney General secured a racketeering and health care fraud...
In late July, a federal district court in Pennsylvania joined in the flurry of False Claims Act (FCA)...
OIG has been busy cracking down on providers who employ or contract with excluded persons or contractors. ...
The owner of a New Jersey ambulance company was indicted for health care fraud in mid-August of...
Our experts at Exclusion Screening, LLC maintain fact sheets that contain the screening requirements...
https://www.exclusionscreening.com/wp-content/uploads/2018/06/Why-do-you-need-a-compliance-Hotline.mp4...
In early August of 2015, the Southern District of New York (SDNY) provided insight as to when the...
The Affordable Care Act (ACA) creates a 60‑day window to report and return overpayments from Medicare...
OIG Audit Findings In a recently released audit, the OIG found that despite the ACA requirement...
DOJ Pursuing Action on Two Separate OIG Exclusion Violations The U.S. Attorney’s Office in Philadelphia...
Assistant Inspector General Testifies before Congress Ann Maxwell, the Assistant Inspector General for...
Exclusion Screening, LLC has been chronicling the Office of Inspector General’s (OIG) interest...
This article was written by Paul Weidenfeld [1] By now, providers should be aware that the Office of...
Exclusion Screening Is Mandatory Providers of medical services that participate in Federal or State Health...
The Department of Justice (DOJ) recently announced two new False Claims Act (FCA) settlements involving...
(This article was originally posted in the National Alliance of Medical Auditing Specialists‘ “Tip...
Home Health Agency Excluded for Employing Excluded Nurse HHS/OIG recently issued a press release announcing...
I. Gains in State Exclusion Enforcement Efforts Highlighted The Office of the Inspector General’s...
Since August 2014, the Office of Inspector General (OIG) has collected roughly $3.75 Million in...
The Office of the Inspector General (OIG) Broadly Interprets Exclusion Regulations OIG’s Demonstrated...
I. Hospital Employed Therapist with Lapsed License The Department of Justice (DOJ) entered...
I. Fraud Found in HHS’ Backyard A Virginia contractor for dental providers was recently indicted...
I. OIG Targets Nursing Homes Last year almost half of the exclusion violation matters reported by the...
I. Excluded Podiatrist Commits Health Care Fraud A Michigan podiatrist who was excluded...
I. Advisory Opinion on Payments for Services Provided Prior to Exclusion The Department of Health...
I. CMPs doubled in OIG Exclusion Violations 2014 Exclusion Screening, LLCSM dedicates a significant...
I. OIG Report In the Office of the Inspector General’s (OIG) semiannual report to Congress,...
Providers are often surprised to learn that a person can be excluded from participation in federal health...
The Office of the Inspector General (OIG) issued a Special Advisory Bulletin in May 2013, which states...

I. Federal and State Agencies Conducting Audits As many healthcare providers and suppliers have painfully...
I. Civil Monetary Penalties Twenty-five out of the fifty-five exclusion enforcement actions reported...
At Exclusion Screening, LLCSM, we know the ins-and-outs of the exclusion screening process. In our opinion,...
I. Mandatory OIG Exclusions When the Office of Inspector General (OIG) considers imposing a mandatory...
I. OIG Recommends Monthly Screening While there is not a formal regulation that mandates monthly...
[visualizer id=”1978″] A quick review of the Office of Inspector General’s (OIG) exclusion...
I. Florida’s State Exclusion. Excluded Providers Costs OIG Over 2.7 Million The Office of...
HHS/OIG Deputy Inspector General Gary Cantrell testified earlier this year that States are failing to...
I. Take It from CMS: If You’re Excluded in One State, You’re Excluded in All States...